



BRI in Pregnancy
Though often unnamed and unrecognized, Bullet Related Injury is a leading, if not THE LEADING, cause of maternal as well as pregnancy-related loss of life.

If you or a loved one have been wounded or threatened, as well as if you have lost someone to a bullet, The BRIC is here for you.
Make an appointment at no charge with
The BRIC for you or your loved ones by clicking below.
For CLINICIANS
BRICare in Pregnancy
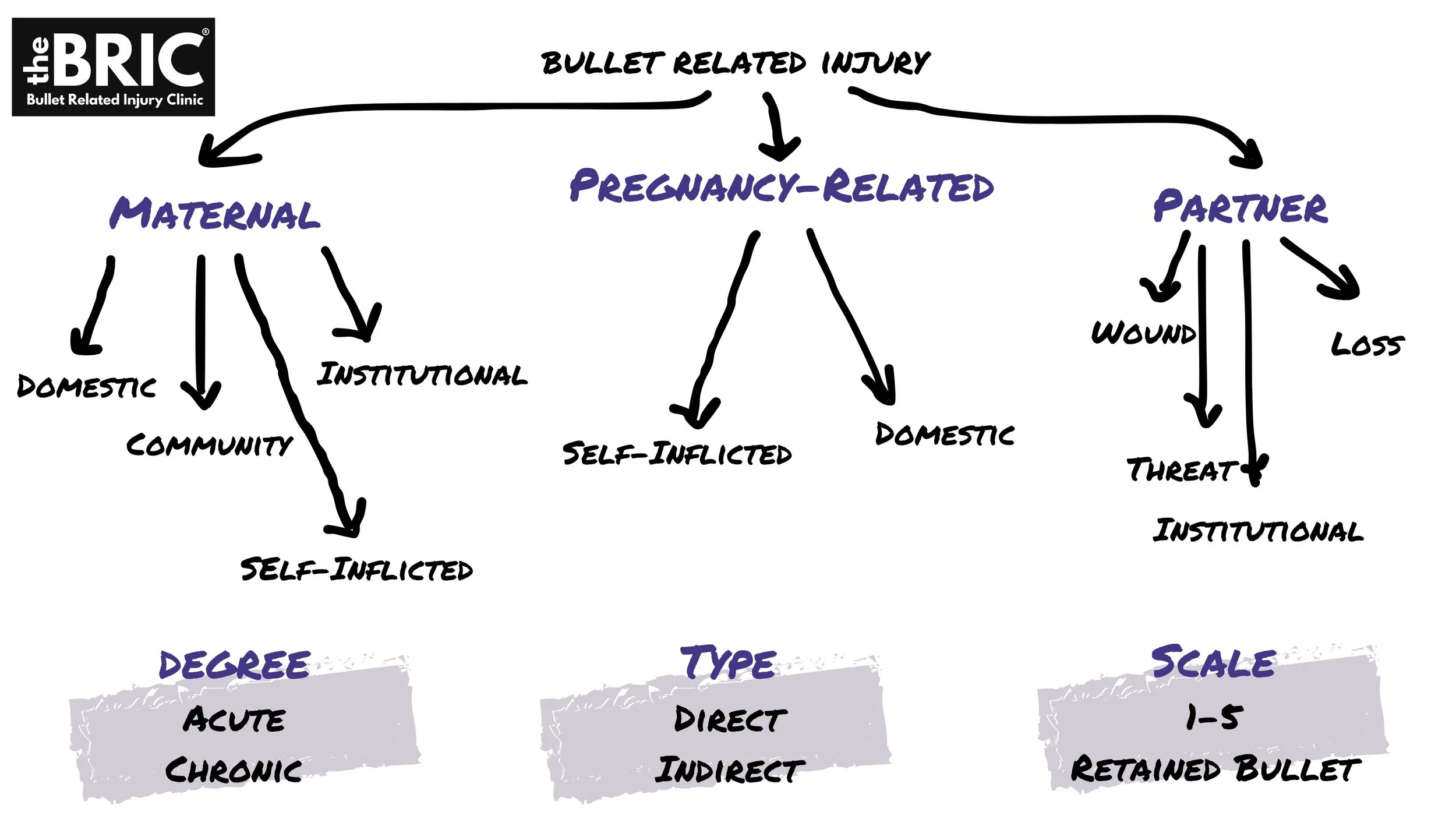
Bullets may impact pregnancy in many ways. Recognizing Bullet Related Injury directly, and indirectly, is essential to caring for and preventing complications of BRI.
DIRECT INJURY
A physical wound is the most readily recognized form of BRI impacting an individual, which includes physical impact of a bullet creating a visible wound. The majority of bullet injury wounds do not require surgery and are not immediately life-threatening, and are therefore often seen as “minor”. However, due to the tremendous transfer of energy into the tissue creating both a path of injury as well as a perimeter of blast effect, often the most severe components of the injury are not immediately apparent. It is as if a tiny bomb has moved through the tissue, so the more tissue that was touched by the bullet’s energy, the more intense the injury. In addition, superficial “graze” wounds are often seen as completely minor, but have a natural history of severe swelling, drainage, and even skin necrosis that can result in a more symptomatic external wound than one that is associated with a “through and through” injury.
Patients often report significant increase in pain associated with their BRI on the days immediately following the day they were injured. This pain experience is largely mediated by inflammation, muscle spasm, and nerve injury, depending on the length of the bullet path as well as the depth the bullet reaches. Wounds that are associated with fractures are also often extremely painful, even when the fracture does not require surgery.
For this reason it is essential to SCALE the injury to allow for appropriate care and guidance in what to expect after the injury has occurred as neuropathic pain and severe muscle spasm are often far worse experiences symptomatically than the external bullet injury wounds themselves.
A uniquely important part of scaling the wound is addressing whether or not there are retained bullets and fragments. The BRIC defines a retained bullet or fragment as anything greater than 5mm in dimension, or about 1/4 inch. Fragments smaller than this are difficult to locate and remove, but are nonetheless very important. The BRIC defines these as “bullet dust” and recommends careful review of all radiographic images and x-rays to assure that full disclosure is given to patients about the extent and nature of their retained bullets. The most definitive guidance comes from a metanalysis of the literature from Dr. Randi Smith in the Journal of Trauma. Patients with bony fractures or multiple RBF, who are at higher risk of elevated BLL, should be monitored for BLL in intervals of 3 months within the first year of injury. For patients who return with BLL above 5 μg/dL, all efforts must be undertaken to remove fragments if there is no potential to worsen the injury.
THREAT
Being threatened with the possibility of a bullet injury can create the same kind of trauma response as actually being injured. This includes being threatened in a domestic setting or by being near a situation where a shooting has occurred. It is important to assess this presentation of BRI and support patients in understanding their trauma. The How2Heal approach takes basic steps toward recognizing and addressing the numerous ways we “have trauma” and what we can do to begin to heal.
INDIRECT INJURY
Indirect injuries occur when someone we know, are close to, live with, care for, or in relationship with has been threatened, wounded, or lost their life to a bullet. There are many ways indirect injury can occur, but one of the most common is having a partner experience an injury during pregnancy. As BRI is the leading cause of death in Black youth and men age 1-44, this makes the overall risk for Indirect BRI higher for Black birthing people. The impact of BRI can be immense, including disruption of safety, economic burdens, disruption of communication, transportation, and housing, and most of all, the presence of a well-regulated partner. The trauma within the body of one person is easily felt within the body of a loved one. This radiating, metastasizing effect often goes completely untreated, in both the person who has been wounded and the loved one. This is due to the fact that 50-70% of BRI is managed only in the ambulatory setting and by very few providers. In this way, the endemic presence of BRI amplifies its effect within pregnancy.
To address discourse around the reality of BRI, the indications for are, and the tools for self-care are invaluable. For this reason The BRIC is working to democratize access to resources or healing.
FATAL INDIRECT BRI
When a pregnant person suffers INDIRECT BRI is fatal, a partner, sibling, child, or parent may have been lost. This acute grief may create undue stress on the person and their loved ones. Recognizing the depth of this injury is essential to supporting patients not just through pregnancy but beyond, as this injury can often manifest as a chronic reality which is present in some form, for a lifetime.
Spiritual care, victim services, mental wellbeing support, child trauma therapy, and ongoing communal care is a mainstay of addressing this loss.
The BRIC has partnered with community based organizations including The Michael Brown JR, Chosen For Change Foundation and their numerous healing events to support those who have lost a loved one to BRI.
